|
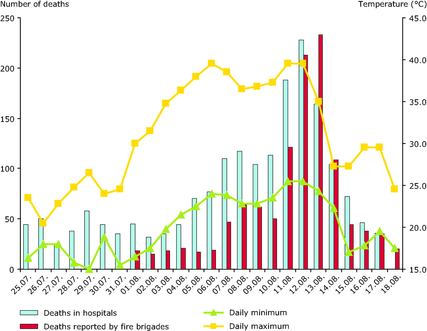
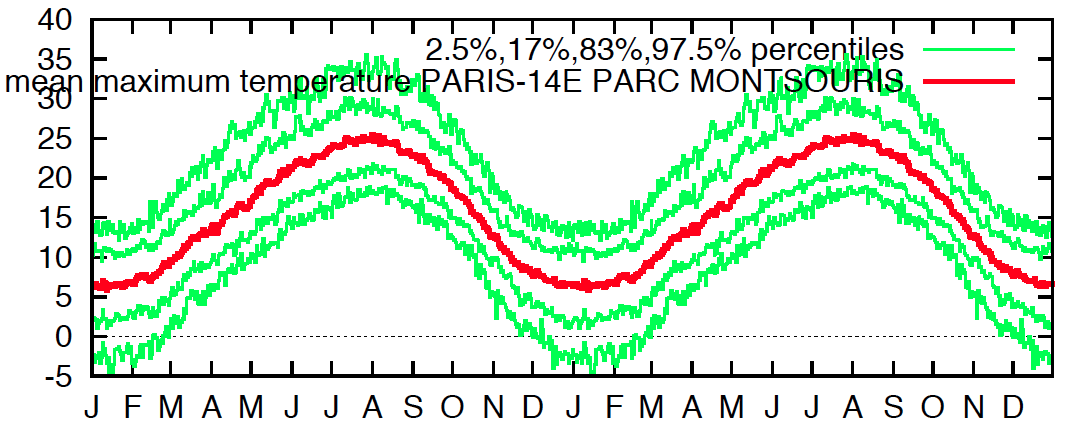
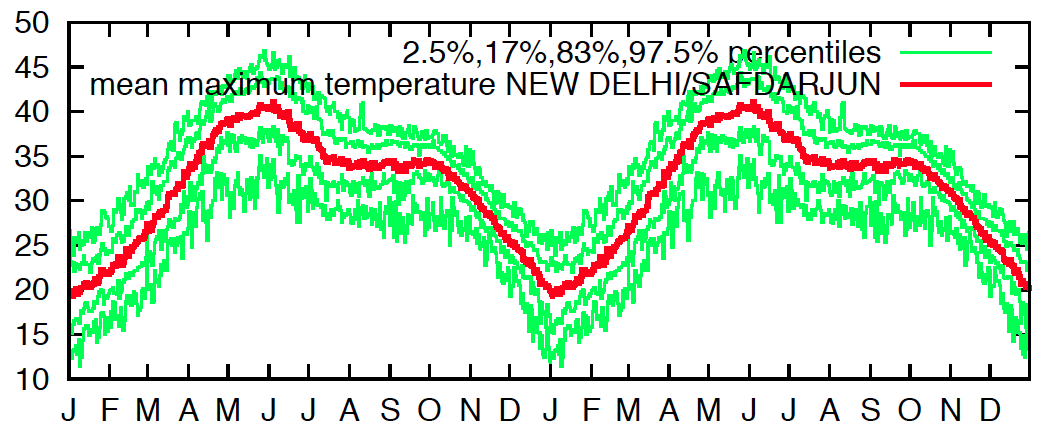
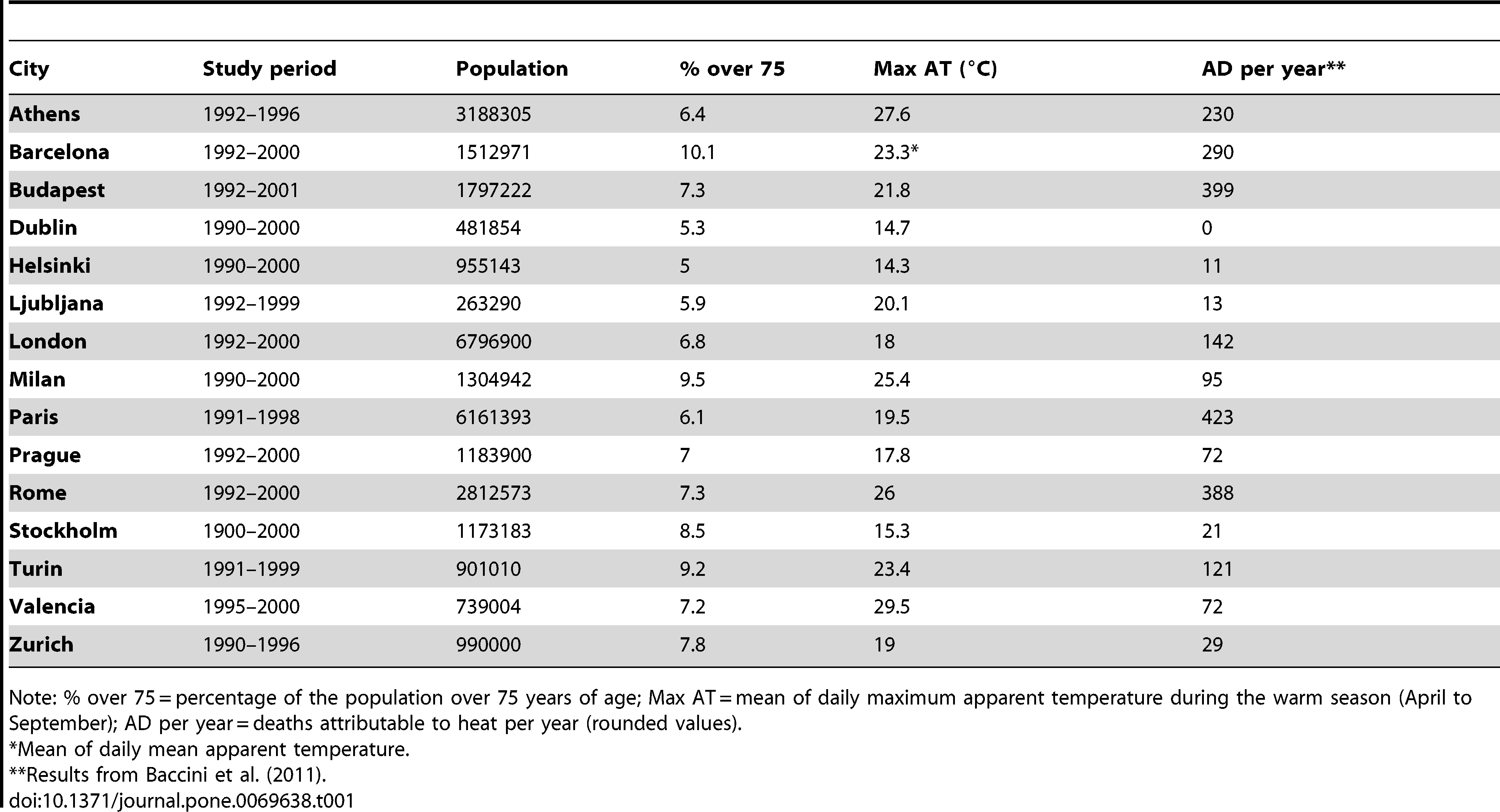
News of recent extreme heat in India ahead of the monsoon, and the associated mortality, brings up reminders of the gripping, society-wide impact such events can have. The term 'harvesting', used to describe long-term reductions in healthy lifespan from a severe event, is an appropriate one. The sheer intensity of the heat also prompts some consideration of the differences in impacts across regions; for instance, in 2003, temperatures in Europe were comparatively cool — peaking close to the early-summer average in New Delhi (see figures below) — and yet mortality was very high, even higher than in this May 2015 Indian heat wave where over a two=week period maximum temperatures averaged around 43 C (109 F) and minimum temperatures around 30 C (86 F). There are of course many differences between the two situations, but the difference in climatological baseline temperatures stands out. Is acclimatization of residents of warm climes a real phenomenon; is it strong enough to account fully for the difference in mortality; and does it imply that percentiles of temperature (i.e. values relative to the local climatology) are of sole importance for determining mortality? These are the multifaceted questions that this post will explore. When it comes to our environments, humans are amazingly adaptable — there's no doubt about that. This is true both on the individual and the species levels. Otherwise we could not have colonized nearly every climatic zone from the tropics to the poles; could not survive on exceedingly variable diets; could not live in city apartment towers when a few short generations ago most of our ancestors lived as peasant farmers on plots thousands of miles away. The only real question, then, concerns the length of the timescale of adaptation to a given perturbation. In biology, this discussion is often framed as a contrast between genetic and epigenetic components (e.g. for adaptation to high altitudes); but those are things that happen over generations or centuries. A study several years ago in Physiological Genomics specified heat acclimatization as "a reversible 'within-lifetime' phenotypic adaptation to long-term elevations in environmental temperature" [emphasis mine]. What can be considered 'long-term' with respect to extreme high temperatures (or any temperatures for that matter)? The answer has bearing on the comparative utility of absolute versus relative measures of temperature-related discomfort: if acclimatization requires a full season or longer to develop, then absolute readings make more sense, whereas shorter and shorter timescales mean relative ones become preferable. If it in fact takes years, the place of one's birth might confer a significant advantage or detriment. Uncertainty on this point is reflected in the National Weather Service's definitions of terms, where a heat wave is simply "uncomfortably hot and humid" but a heat advisory is issued at specific temperature thresholds independent of the location's climatology.
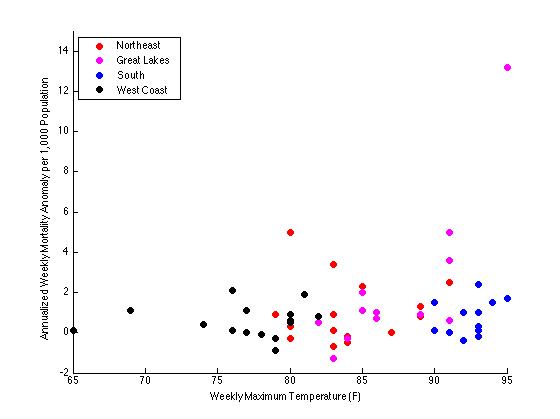
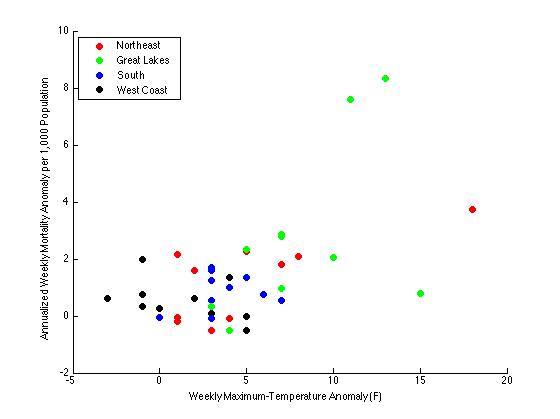
What does the literature say? Several studies looking at this question have in fact determined that the 'exposure-response' curve for temperature and mortality does shift with the underlying climatology. One study in Europe found that the daily-temperature threshold above which deaths begin to significantly increase is 29 deg C in the Mediterranean region versus 23 deg C in northern areas. However, with a higher absolute tolerance comes a greater increase in deaths per degree C above the threshold — 3.1% vs. 1.8%. Similarly, in Alabama defining heat waves in terms of percentiles relative to the climatology yielded the best match with excess-mortality figures. Altogether, the relationship between high temperatures and mortality seems to be stronger in cooler regions — a 'heat-wave effect' of 6.8% higher non-accidental mortality during heat waves in the Northeast U.S., but only 1.8% in the South. (However, these numbers are not significantly different at the 95th percentile.) In fact, recognition of these climate-mediated differences goes back all the way to some of the earliest papers on the subject, such as a study published in Public Health Reports in 1938. Among noteworthy findings like a 70% increase in total mortality during and immediately following the peak of the record-setting July 1936 heat wave (also see here), and a greater incidence of mortality in cities than in rural areas, the author observed that excess mortality was higher in the North despite being cooler than the South, and therefore that it seemed to be associated primarily with the temperature anomaly rather than the absolute temperature. A quick plotting of the data tables from that paper helps in visualizing the basis for this conclusion (see below). Note that in a more careful analysis many corrections would be made that would most likely narrow the conditional spread, e.g. considering in a more-sophisticated way the delayed response of mortality to temperature; using percentiles rather than the numerical anomaly; correlating with a combination of the anomaly and the absolute value; etc.
Of course it's not just acclimatization that could explain regional variations in the mortality response: societal and personal awareness translated into preventive measures (e.g. wearing loose clothing, not exercising in the heat of the day, managing household airflow) maps onto the differing availability of cooling technology. But the 1938 study, predating as it does the mass adoption of A/C, suggests that while A/C may have reduced overall heat-related mortality, its effect was not to increase vulnerability in cool climates relative to warm ones where its use is now more widespread. Not ruled out, though, are design features like the large porches and generally more-open, low-density patterns of settlement in the southern U.S. vis-à-vis the North (especially in the past). On the other hand, it has been reported that heat stroke is more prevalent in Arabia than in North America — but it is unclear to what extent this is affected by influxes of pilgrims during the Hajj. Finally, regarding the timescale of acclimatization, a number of studies have shown that mortality is highest in the first heat wave of the summer; evidence points to a combination of a lack of acclimatization in the population and to the deaths of the most susceptible inflating the early-season numbers. That same study notes a specific figure of several weeks — short enough to be consistent with a intra-season decline in sensitivity for a fixed population, but too long to be of great help to pilgrims to the sweltering deserts of Saudi Arabia. A breakdown of Hajj heat-related mortality by country of origin would be an interesting way to further examine this.
So, to resolve the initial motivating questions: acclimatization is real, and it is likely by itself to account for a significant fraction of the reduced mortality of residents of warm regions relative to cool ones when confronted with the same ambient temperatures. It is not clear if this is true throughout the temperature spectrum (e.g. in the subtropical deserts); at least one study has suggested there is a hard upper temperature limit on the body's ability to function. At the other extreme, although percentiles seem in general to be better predictors of excess mortality than absolute values, no one suffers from heat in Ireland (never mind the Arctic). In the climate literature, little work has been devoted to controlling for other societal and cultural factors influencing the population's exposure and physiological-adaptation capabilities. These have been implicated in many of the 2003 heat-wave deaths in France (such as sleeping on hot upper floors of houses), so they are nontrivial in understanding inter-regional differences. Acclimatization timescales are in some sense mirrored in the non-instantaneous nature of heat-related mortality — perhaps the most apt analogy (almost equivalence) is that of a disease, where immunity is nice but only if one survives to reap its benefits. Nature abhors a discontinuity, so ideally the body would take a week or so of adjustment time to a hot climate or vigorous exercise in the heat. In other words, in the context of a trip to India in May, three of these precautions apply to the climate as well as to the food.
0 Comments
Leave a Reply. |
Archives
September 2023
Categories |
 RSS Feed
RSS Feed
{kind=link}